
Why weight loss is harder when you have ADHD


Why weight loss is harder when you have ADHD
June 9, 2026 by addrc
Harold Robert Meyer -The ADD Resource Center
www.addrc.org
Reviewed: June 3, 2026 Published: June 6.2026
Listen to understand, not just to respond
If you have ADHD and your weight keeps climbing no matter how hard you try, you are not lazy and you are not failing. Research consistently shows that people with ADHD are far more likely to struggle with weight than their peers — and the reasons are wired into how the ADHD brain handles reward, impulse, and routine. Understanding those mechanisms is the first step toward strategies that actually work for you.
Key takeaway
Weight is harder to manage with ADHD because the same brain differences that drive inattention and impulsivity — especially in the dopamine reward system — also push you toward eating for stimulation, eating impulsively, and struggling with the planning that consistent eating requires. The challenge is neurological, not a matter of discipline. Once you treat it as a brain-based pattern rather than a personal failing, the right tools — behavioral, medical, and sometimes pharmacological — become far more effective.
Why this matters
Excess weight rarely travels alone. It raises the risk of type 2 diabetes, heart disease, sleep problems, and depression — conditions that already shadow many people with ADHD. When weight struggles are misread as laziness, shame compounds, motivation collapses, and the cycle tightens. Treating the ADHD–weight link as the medical pattern it is changes everything: it opens the door to approaches that fit how your brain actually works, and it replaces self-blame with strategies you can sustain over time.
Key findings
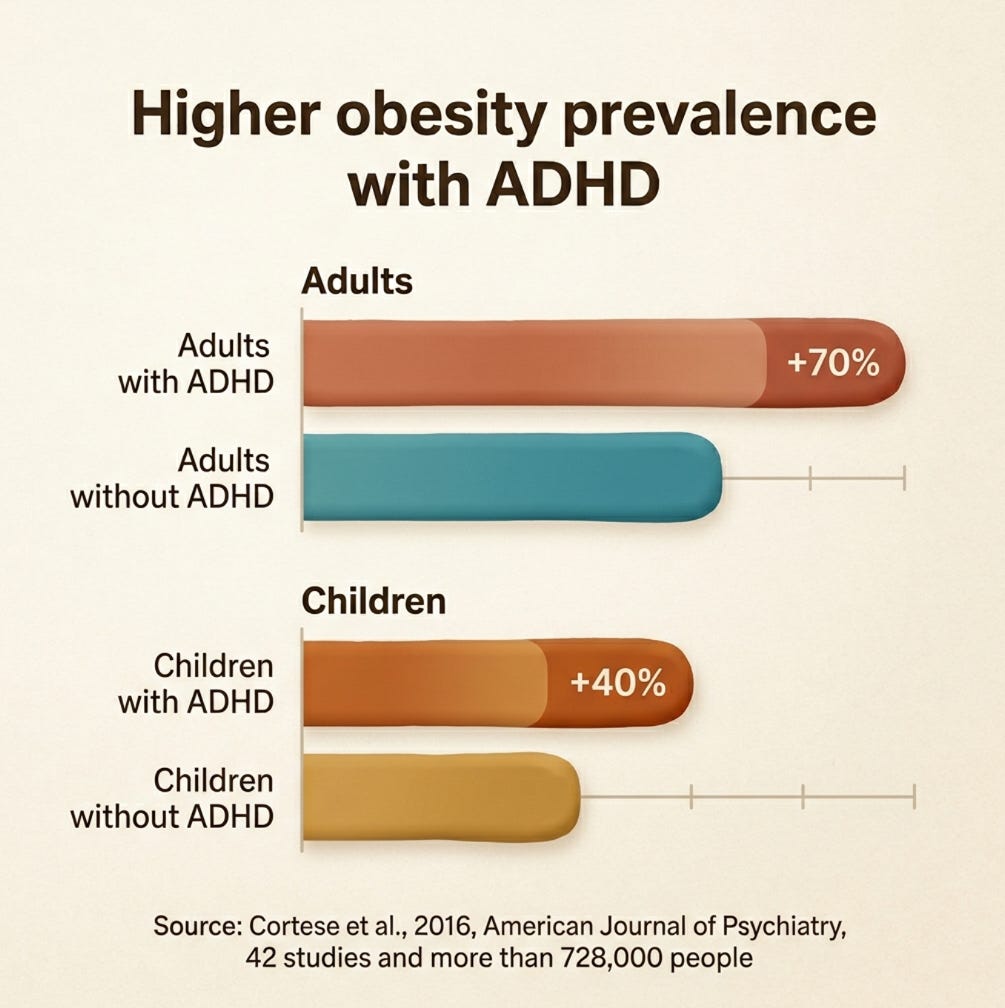
Adults with ADHD have roughly 70% higher obesity prevalence, and children about 40% higher, than peers without ADHD, according to a meta-analysis of 42 studies covering more than 728,000 people (Cortese et al., 2016, American Journal of Psychiatry).
Lower dopamine signaling drives the ADHD brain to seek stimulation, and food — especially sugar and refined carbohydrates — delivers a fast, easy dopamine reward.
People with ADHD tend to eat more junk food and ultra-processed food and fewer fruits, vegetables, and whole foods — diets engineered to be fast, cheap, and intensely rewarding (Pediatric Research, 2026).
Impulsivity and executive-function gaps make meal planning, portioning, and eating on a regular schedule genuinely harder, as covered in the ADDRC guide to binge eating and ADHD.
GLP-1 weight-loss drugs such as semaglutide and tirzepatide can help with weight but do not treat ADHD, and combining them with stimulants requires medical monitoring.
The dopamine connection
The ADHD brain tends to run low on dopamine, the neurotransmitter that governs reward and motivation. To compensate, it keeps reaching for stimulation — and food is one of the fastest, cheapest sources around. Sugar and refined carbohydrates trigger a quick dopamine surge, which is exactly why they are so easy to overeat when you are bored, stressed, or under-stimulated. This shows up in what people with ADHD actually eat: research finds they tend to consume more junk food and ultra-processed food — and fewer fruits, vegetables, and whole foods — than their peers (Pediatric Research, 2026). Those products are formulated to be fast, cheap, and intensely rewarding, which makes them a near-perfect match for a brain hunting stimulation. A 2016 review in the American Journal of Psychiatry found obesity prevalence roughly 70% higher in adults with ADHD, and longitudinal evidence increasingly points to ADHD playing a causal role in weight gain rather than the two simply coexisting.
“People with ADHD often aren’t eating because they’re hungry,” notes Harold Robert Meyer of The ADD Resource Center. “They’re eating because the brain is asking for a hit of stimulation, and food answers faster than almost anything else.”
It is not willpower — it is executive function
Losing weight assumes a working set of executive skills: planning meals, shopping ahead, portioning, noticing hunger and fullness, and staying consistent day after day. These are precisely the skills ADHD disrupts. The result is a familiar pattern — skipping meals while hyperfocused, then ravenous overeating later; grabbing convenience food because nothing was prepped; or eating impulsively in the evening when structure and mental energy are lowest. As the ADDRC guide to binge eating and ADHD explains, this is not weak character. It is the predictable outcome of a brain that struggles with delay, planning, and impulse control. Rigid diets that demand detailed tracking and exact portions tend to fail people with ADHD for the same reason — they lean on the very functions that are impaired. The ADDRC overview of ADHD and obesity covers practical alternatives in more depth.
The weight-loss-drug question
GLP-1 receptor agonists — semaglutide (sold as Ozempic for diabetes and Wegovy for weight management) and tirzepatide (Mounjaro and Zepbound) — have reshaped the weight-loss conversation. They reduce appetite, slow stomach emptying, and can produce significant, sustained weight loss. But two things are essential to understand.
First, these drugs are not approved to treat ADHD and there is no robust evidence yet that they improve ADHD symptoms. Some early research suggests that GLP-1 signaling affects dopamine and reward pathways, but that work is mostly preliminary — animal models and small studies — and should not be read as evidence for attention or focus benefits.
Second, people with ADHD can use GLP-1 medications for weight management, but combining them with stimulants calls for monitoring. Both stimulants and GLP-1 drugs suppress appetite, so under-eating and poor nutrition are real risks. Because GLP-1s slow gastric emptying, they can also affect how oral extended-release ADHD medications are absorbed, and both can influence blood pressure and heart rate. Separately, the stimulant lisdexamfetamine (Vyvanse) is FDA-approved for binge-eating disorder, which sometimes overlaps with ADHD. None of this is do-it-yourself territory — every combination should be managed by your prescriber.
What actually helps
Treat the ADHD first. When core symptoms are managed, impulsive and disorganized eating often eases. Then build structure that does not depend on willpower: consistent meal and snack times so extreme hunger never sets up a binge, protein at each eating occasion, and removing friction by keeping easy, satisfying whole-food options within reach so the convenient choice is also the better one. Choose movement you genuinely enjoy rather than punishing routines, and set small, specific, frequent wins — because a dopamine-driven brain responds to wins it can actually feel.
“Stop trying to out-discipline your biology,” says Meyer. “Design your environment so the easy choice is the good one, and let your brain coast downhill instead of fighting uphill.”
Bibliography
Cortese, S., Moreira-Maia, C. R., St. Fleur, D., Morcillo-Peñalver, C., Rohde, L. A., & Faraone, S. V. (2016). Association between ADHD and obesity: A systematic review and meta-analysis. American Journal of Psychiatry, 173(1), 34–43. https://psychiatryonline.org/doi/10.1176/appi.ajp.2015.15020266
Cortese, S. (2019). The association between ADHD and obesity: Intriguing, progressively more investigated, but still puzzling. Brain Sciences, 9(10), 256. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6826981/
Cortese, S., & Tessari, L. (2017). Attention-deficit/hyperactivity disorder (ADHD) and obesity: Update 2016. Current Psychiatry Reports, 19(1), 4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5247534/
Attention-deficit/hyperactivity disorder is associated with increased consumption of ultra-processed foods among children. (2026). Pediatric Research. https://www.nature.com/articles/s41390-026-04844-5
Resources
“ADHD and obesity: Understanding the connection and what you can do about it” — https://www.addrc.org/adhd-and-obesity-understanding-the-connection-and-what-you-can-do-about-it/
“Binge eating and ADHD: Understanding and managing the cycle” — https://www.addrc.org/binge-eating-and-adhd-understanding-and-managing-the-cycle/
“Explore more at the ADD Resource Center” —
https://www.addrc.org
U.S. Food and Drug Administration — drug information on approved medications —
https://www.fda.gov
What’s next
Bring this to a conversation with your clinician rather than another solo attempt at sheer discipline. Ask whether treating your ADHD more effectively could be the missing piece, and if weight is a medical concern, ask about all the tools available — behavioral, medical, and pharmacological — and how they fit your situation. Start with one small, specific change this week. For more practical, brain-based guidance, visit
https://www.addrc.org/
.
About the author
Harold Meyer founded The ADD Resource Center in 1993 and has spent more than 30 years translating the lived experience of ADHD into practical guidance for individuals and the professionals who support them. He co-founded CHADD of New York and led the Institute for the Advancement of ADHD Coaching. An author and international speaker, he has presented at the American Psychiatric Association Annual Meeting, CHADD national and local conferences, NYU Langone, Mount Sinai Medical Center, and Weill Cornell Medical College. Reach him at haroldmeyer@addrc.org.
info@addrc.org • +1 (646) 205-8080 • 127 West 83rd St., Unit 133, Planetarium Station, New York, NY 10024-0840 USA • X | LinkedIn | Substack | ADHD Research and Innovation
Join our community — Subscribe to the ADD Resource Center newsletter for the latest resources and insights → Click here.
Content disclaimer: Our content is intended for educational and informational purposes only and does not replace professional advice. While we strive for accuracy, mistakes or omissions may occur. Some content may be partially generated by artificial intelligence tools, which can lead to inaccuracies. Readers should verify the information themselves. Rejection Sensitive Dysphoria (RSD) is recognized by many providers but is not in the DSM.
Crisis line: In the USA and Canada, call or text 988 anytime for free mental health and suicide prevention support.
Privacy & legal: Under GDPR and CCPA, you may request access to, correction of, or deletion of your personal data at info@addrc.org.
©2026 Harold R. Meyer / The ADD Resource Center. All rights reserved. Content may be shared only in complete, unaltered form with attribution. Reproduction or commercial use requires written permission at addrc@mail.com.